| disorders_of_the_nervous_system_ns_2013.pptx |
Objective #17
Anaesthetic Drugs
-- 2 types – general and local
Local
– numb a small area (novocaine – tooth pulled; lidocaine - shingles)
–Blocks passage of nerve impulse from skin to the brain
–Disrupts the sodium channels – these are needed for action potential to occur
General
– patient is sometimes unconscious and feels no pain.
-Example N20 –laughing gas
-Major surgery, wisdom teeth removed, c-section.
-Ex. Ether – disrupts proteins in cell membranes
-Barbituates (sleeping pills) enhance neurotransmitter activity (GABA – inhibitory neurotransmitter)
Depressants
– slow down CNS – relaxes, less pain, reduced coordination and judgement
Legal Illegal Prescription
Alcohol Marijuana *sometimes prescribed Morphine
Valium
oxycontin
Stimulants
– speed up the CNS – increased energy and confidence; sometimes paranoia
Legal Illegal Prescription
caffeine cocaine Ritalin
nicotine ecstasy
** also refer to handout on Drugs and their effects
Drugs and Their Effects
Depressants (DOVAM)
Oxycontin (Opioid)
attach to opioid receptors
block transmission of pain messages to the brain and causes respiratory depression
can produce feeling of euphoria by affecting pleasure regions of the brain
Valium (CNS depressant)
slow normal brain function
affects GABA neurotransmitter - GABA functions to decrease brain activity
increased doses of Valium result in drowsiness... helps treat anxiety and sleep disorders
Alcohol
depressant, but can act as stimulant in small doses
increases inhibitory neurotransmitter GABA (most common inhibitory in brain)
modifies effects of glutamate (75% of all excitatory responses)
Marijuana
Binds to receptors found on presynaptic membranes in the brain
receptors function in blunting pain
causes release of neurotransmitter dopamine - elevates mood and controls
muscle movements
can cause euphoria in small doses; blocks pain, frustration and
confusion
Stimulants (SCERN)
Cocaine
stimulating the release of norepinephrine and dopamine
in higher does stimulates the release of serotonin
interferes with re-uptake of these neurotransmitters... therefore they build up in synapse
over time, body produces less dopamine and more cocaine will be needed for
same effect
Caffeine
blocks inhibitory receptors - don’t get the inhibitory response - stimulant
when injected in experimental conditions, subjects reported a ‘high’ similar to cocaine
Ecstasy
increasing the activity of serotonin, dopamine, and norepinephrine (more effects on serotonin)
causes damage to brain cells that produce serotonin
Ritalin (Stimulant)
Used to treat attention deficit hyperactivity disorder
enhance brain activity, resulting in increased alertness and energy
increase the amounts of norepinephrine and dopamine neurotransmitters
Nicotine
affects CNS and PNS; stimulates dopamine
increases arousal level in brain (stimulant) although people report that it ‘relaxes’ them
REFER TO WEBSITES SECTION FOR LONG AND SHORT TERM EFFECTS OF CAFFEINE AND NICOTINE (THE OTHERS ARE BELOW)
Anaesthetic Drugs
-- 2 types – general and local
Local
– numb a small area (novocaine – tooth pulled; lidocaine - shingles)
–Blocks passage of nerve impulse from skin to the brain
–Disrupts the sodium channels – these are needed for action potential to occur
General
– patient is sometimes unconscious and feels no pain.
-Example N20 –laughing gas
-Major surgery, wisdom teeth removed, c-section.
-Ex. Ether – disrupts proteins in cell membranes
-Barbituates (sleeping pills) enhance neurotransmitter activity (GABA – inhibitory neurotransmitter)
Depressants
– slow down CNS – relaxes, less pain, reduced coordination and judgement
Legal Illegal Prescription
Alcohol Marijuana *sometimes prescribed Morphine
Valium
oxycontin
Stimulants
– speed up the CNS – increased energy and confidence; sometimes paranoia
Legal Illegal Prescription
caffeine cocaine Ritalin
nicotine ecstasy
** also refer to handout on Drugs and their effects
Drugs and Their Effects
Depressants (DOVAM)
Oxycontin (Opioid)
attach to opioid receptors
block transmission of pain messages to the brain and causes respiratory depression
can produce feeling of euphoria by affecting pleasure regions of the brain
Valium (CNS depressant)
slow normal brain function
affects GABA neurotransmitter - GABA functions to decrease brain activity
increased doses of Valium result in drowsiness... helps treat anxiety and sleep disorders
Alcohol
depressant, but can act as stimulant in small doses
increases inhibitory neurotransmitter GABA (most common inhibitory in brain)
modifies effects of glutamate (75% of all excitatory responses)
Marijuana
Binds to receptors found on presynaptic membranes in the brain
receptors function in blunting pain
causes release of neurotransmitter dopamine - elevates mood and controls
muscle movements
can cause euphoria in small doses; blocks pain, frustration and
confusion
Stimulants (SCERN)
Cocaine
stimulating the release of norepinephrine and dopamine
in higher does stimulates the release of serotonin
interferes with re-uptake of these neurotransmitters... therefore they build up in synapse
over time, body produces less dopamine and more cocaine will be needed for
same effect
Caffeine
blocks inhibitory receptors - don’t get the inhibitory response - stimulant
when injected in experimental conditions, subjects reported a ‘high’ similar to cocaine
Ecstasy
increasing the activity of serotonin, dopamine, and norepinephrine (more effects on serotonin)
causes damage to brain cells that produce serotonin
Ritalin (Stimulant)
Used to treat attention deficit hyperactivity disorder
enhance brain activity, resulting in increased alertness and energy
increase the amounts of norepinephrine and dopamine neurotransmitters
Nicotine
affects CNS and PNS; stimulates dopamine
increases arousal level in brain (stimulant) although people report that it ‘relaxes’ them
REFER TO WEBSITES SECTION FOR LONG AND SHORT TERM EFFECTS OF CAFFEINE AND NICOTINE (THE OTHERS ARE BELOW)
Objective 18
Biology 3201
Use of Drugs for Nervous System Disorders vs. Long Term Effects
Clinical Depression
• fault in brain chemistry dealing with serotonin, dopamine, or noradrenaline
• Drugs: serotonin reuptake inhibitors (SSRI’s), MAOI’s and Tricyclic Compounds
• Tricyclic Inhibitors slow the reuptake of Serotonin and Noradrenaline
• MAOI’s inhibit Monoamine Oxidase (MAO) - enzyme that breaks down serotonin and noradrenaline
• increase in these neurotransmitters elevates mood
• Danger of MAOI’s:
1. Increased risk of heart failure
2. Cannot be taken with certain foods (cause increase blood pressure, heart failure and death)
3. Lethal at low doses... concern for suicidal patients
• SSRI’s are most widely used, as they have fewer dangerous side-effects
• Ex. Prozac
• Side effects: nausea, headache, insomnia and anxiety
Bipolar Disorder
• severe mood swings resulting in a manic and depressive phase
• Meds: lithium bicarbonate
• prevents mood swings
• taken during manic phase
• depressive phase is a result of the manic phase
• controlling the manic phase indirectly controls the depressive phase
• long term use: problems with kidney and thyroid (interferes with water and salt balance)
• other side effects: diarrhea, nausea, hand tremor, blurred vision, confusion, and leg and feet swelling
• uncomfortable side effects reason why people stop using lithium even if they need it
Schizophrenia
• excessive dopamine activity (excess number of dopamine receptors)
• Meds: Chlorpromazine
• blocks dopamine receptors
• Side effects: similar to Parkinson’s
• Others: abnormal body and face movements, extreme pacing, dry mouth, constipation, blurred vision, and low blood pressure
Problems with most of these drugs is that the drug necessary to help them function normally in society has difficult side effects.
Biology 3201
Use of Drugs for Nervous System Disorders vs. Long Term Effects
Clinical Depression
• fault in brain chemistry dealing with serotonin, dopamine, or noradrenaline
• Drugs: serotonin reuptake inhibitors (SSRI’s), MAOI’s and Tricyclic Compounds
• Tricyclic Inhibitors slow the reuptake of Serotonin and Noradrenaline
• MAOI’s inhibit Monoamine Oxidase (MAO) - enzyme that breaks down serotonin and noradrenaline
• increase in these neurotransmitters elevates mood
• Danger of MAOI’s:
1. Increased risk of heart failure
2. Cannot be taken with certain foods (cause increase blood pressure, heart failure and death)
3. Lethal at low doses... concern for suicidal patients
• SSRI’s are most widely used, as they have fewer dangerous side-effects
• Ex. Prozac
• Side effects: nausea, headache, insomnia and anxiety
Bipolar Disorder
• severe mood swings resulting in a manic and depressive phase
• Meds: lithium bicarbonate
• prevents mood swings
• taken during manic phase
• depressive phase is a result of the manic phase
• controlling the manic phase indirectly controls the depressive phase
• long term use: problems with kidney and thyroid (interferes with water and salt balance)
• other side effects: diarrhea, nausea, hand tremor, blurred vision, confusion, and leg and feet swelling
• uncomfortable side effects reason why people stop using lithium even if they need it
Schizophrenia
• excessive dopamine activity (excess number of dopamine receptors)
• Meds: Chlorpromazine
• blocks dopamine receptors
• Side effects: similar to Parkinson’s
• Others: abnormal body and face movements, extreme pacing, dry mouth, constipation, blurred vision, and low blood pressure
Problems with most of these drugs is that the drug necessary to help them function normally in society has difficult side effects.
Objective 20 - How the eye maintains homeostasis
•Use your eyes to respond to changes in your environment.
Ex. •Pupil is adjusted based on the amount of light
•Interpret information we see.
Ex. •Lens adjusts as you look close up or far away
•Rods and cones used at different light levels so you can still see.
•Tears – flushing things out of your eye
•Blinking – keeping your eyes moist
•Use your eyes to respond to changes in your environment.
Ex. •Pupil is adjusted based on the amount of light
•Interpret information we see.
Ex. •Lens adjusts as you look close up or far away
•Rods and cones used at different light levels so you can still see.
•Tears – flushing things out of your eye
•Blinking – keeping your eyes moist
Objective 21.
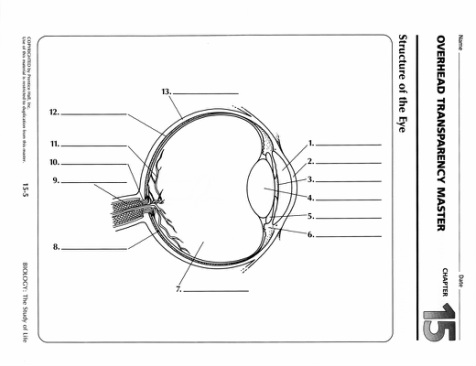
The Human Eye
(p.409-13) - protected by eyelashes,
eyelids, eyebrows, and ridge of bone in the
skull.
Structures and functions: (Refer to Figure 12.19 p. 410)
Three layers of the eye include:
A. sclera -> thick, white, outer layer that gives the eye its shape.
B. cornea -> at the front of the eye, the sclera bulges forward, and becomes clear.
C. choroid layer -> middle, coloured layer; absorbs light not absorbed by the sclera, and prevents internal reflection.
Iris -> at front of the eye, the choroid becomes the iris; opens and closes to regulate the amount of light entering the eye.
Pupil -> the aperture (hole) in the middle of the iris. Pupil is
large in dim light and small in bright light.
Lens -> a clear, flexible, crystalline structure that changes shape allowing the focussing of an image on the retina at the back of the eye. The lens is attached to suspensory ligaments, which, in turn, are attached to a ciliary body, containing muscles that contract and relax to change the lens
shape.
(See Figure 12.21 p. 412)
- lens is long and thin -> focus a distant object ( relaxed ciliary muscle causes suspensory ligaments to tighten)
- lens short and rounded (accommodation); focuses a near object. ( contracted ciliary muscles causing suspensory ligaments to relax.)
Retina -> inner layer of the eye on which image forms (inverted and reversed) from the lens.
- contains three layers:
a. rod and cone layer (make up inside layer of retina)
Rods - composed of two types of photoreceptors (sensory)
- is sensitive to even dim light and so is useful for night vision,
- is unable to distinguish colors (only shades of gray)
Cones- stimulated in bright light
- can distinguish colors, so is useful for daytime vision.
b. bipolar cell layer (middle layer of retina)
- synapses with rods or cones and transmits impulses to ganglion cell layer.
c. ganglion cell layer (outside layer of retina)
- ganglion cells join together to form optic nerve that transmits impulses to the occipital lobe of the brain where the info is interpreted and we see.
Fovea centralis - area in the retina that lies directly behind the center of the lens.
- cones are concentrated here, allowing a very distinct image (fine detail)
Blind spot - area of the retina where optic nerve forms.
- no rods or cones here, so any image that falls on this area of the retina is not transmitted to the brain.
Anterior chamber - small area between the cornea and the lens
- filled with a fluid called aqueous humor.
- together with cornea acts as a prelens to initiate focussing of the image.
Posterior chamber
- larger area between the lens and the retina
- filled with a clear gel called vitreous humor.
- helps to maintain the shape of the eyeball
The Human Eye
(p.409-13) - protected by eyelashes,
eyelids, eyebrows, and ridge of bone in the
skull.
Structures and functions: (Refer to Figure 12.19 p. 410)
Three layers of the eye include:
A. sclera -> thick, white, outer layer that gives the eye its shape.
B. cornea -> at the front of the eye, the sclera bulges forward, and becomes clear.
C. choroid layer -> middle, coloured layer; absorbs light not absorbed by the sclera, and prevents internal reflection.
Iris -> at front of the eye, the choroid becomes the iris; opens and closes to regulate the amount of light entering the eye.
Pupil -> the aperture (hole) in the middle of the iris. Pupil is
large in dim light and small in bright light.
Lens -> a clear, flexible, crystalline structure that changes shape allowing the focussing of an image on the retina at the back of the eye. The lens is attached to suspensory ligaments, which, in turn, are attached to a ciliary body, containing muscles that contract and relax to change the lens
shape.
(See Figure 12.21 p. 412)
- lens is long and thin -> focus a distant object ( relaxed ciliary muscle causes suspensory ligaments to tighten)
- lens short and rounded (accommodation); focuses a near object. ( contracted ciliary muscles causing suspensory ligaments to relax.)
Retina -> inner layer of the eye on which image forms (inverted and reversed) from the lens.
- contains three layers:
a. rod and cone layer (make up inside layer of retina)
Rods - composed of two types of photoreceptors (sensory)
- is sensitive to even dim light and so is useful for night vision,
- is unable to distinguish colors (only shades of gray)
Cones- stimulated in bright light
- can distinguish colors, so is useful for daytime vision.
b. bipolar cell layer (middle layer of retina)
- synapses with rods or cones and transmits impulses to ganglion cell layer.
c. ganglion cell layer (outside layer of retina)
- ganglion cells join together to form optic nerve that transmits impulses to the occipital lobe of the brain where the info is interpreted and we see.
Fovea centralis - area in the retina that lies directly behind the center of the lens.
- cones are concentrated here, allowing a very distinct image (fine detail)
Blind spot - area of the retina where optic nerve forms.
- no rods or cones here, so any image that falls on this area of the retina is not transmitted to the brain.
Anterior chamber - small area between the cornea and the lens
- filled with a fluid called aqueous humor.
- together with cornea acts as a prelens to initiate focussing of the image.
Posterior chamber
- larger area between the lens and the retina
- filled with a clear gel called vitreous humor.
- helps to maintain the shape of the eyeball
Objective 22
Path of Light through the eye - cornea -> aqueous humour (anterior compartment) -> pupil -> lens -> vitreous humour (posterior compartment -> retina -> optic nerve
Path of Light through the eye - cornea -> aqueous humour (anterior compartment) -> pupil -> lens -> vitreous humour (posterior compartment -> retina -> optic nerve
Objective 23 - Eye Disorders
Disorders of the Eye
1. cataracts - cloudy or opaque areas on the lens that increase over time, eventually causing blindness. - tend to occur in older
people and exposure to sunlight
- treated by surgically replacing the lens with an artificial lens
2. glaucoma - buildup of excessive aqueous humor between the lens and the cornea.
- fluid drainage system becomes blocked, pressure build todestroy nerve fibres responsible for peripheral (side)vision.
- cannot be repaired, but can be curbed with drugs and surgery. (eye checkups **)
3. myopia (nearsightedness) See Figure 12.22 p. 414
- difficulty seeing things far away
- shape of eyeball too long or ciliary muscle too strong.
- corrective concave lens corrects by making focal point longer.
4. hyperopia (farsightedness)
- difficulty seeing things close up
- shape of eyeball too short or ciliary muscle too weak to focus image of nearby object onto the retina.
- corrective convex lens makes focal point shorter.
5. Astigmatism
- abnormal shape of the cornea or lens resulting in uneven focus.
- uneven corrective lens allows clear vision.
Objective 24 - Means of correcting eye disorders
In some cases, myopia, hyperopia and astigmatism can be corrected with surgery known as laser refractive correction.
Two main types:
a. photorefractive keratectomy (PRK)
- outpatient procedure performed with local anaesthetic eye drops.
- laser beam reshapes the cornea by cutting microscopic amounts of tissue from the corna's outer surface.
- takes a few minutes / quick recovery
- controlled by computer
b. laser in situ keratomileusis (LASIK)
- more complex
- performed for nearsightedness
- knife removes a flap of corneal tissue, laser removes tissue underneath, and the corneal flap is replaced.
- depends on surgeon's skill (NOTE: NOWADAYS CAN BE PERFORMED ENTIRELY BY LASER AS WELL)
Both procedures have high success rates; in some cases, however, eyesight diminishes after surgery.
Impaired cornea - usually caused by disease
- corneal transplant from donor performed
- no need for type-matching
- recovery long; vision improves gradually 6-12 mths.
Clear Lens Replacement - refer to class handout - used to treat cataracts
Disorders of the Eye
1. cataracts - cloudy or opaque areas on the lens that increase over time, eventually causing blindness. - tend to occur in older
people and exposure to sunlight
- treated by surgically replacing the lens with an artificial lens
2. glaucoma - buildup of excessive aqueous humor between the lens and the cornea.
- fluid drainage system becomes blocked, pressure build todestroy nerve fibres responsible for peripheral (side)vision.
- cannot be repaired, but can be curbed with drugs and surgery. (eye checkups **)
3. myopia (nearsightedness) See Figure 12.22 p. 414
- difficulty seeing things far away
- shape of eyeball too long or ciliary muscle too strong.
- corrective concave lens corrects by making focal point longer.
4. hyperopia (farsightedness)
- difficulty seeing things close up
- shape of eyeball too short or ciliary muscle too weak to focus image of nearby object onto the retina.
- corrective convex lens makes focal point shorter.
5. Astigmatism
- abnormal shape of the cornea or lens resulting in uneven focus.
- uneven corrective lens allows clear vision.
Objective 24 - Means of correcting eye disorders
In some cases, myopia, hyperopia and astigmatism can be corrected with surgery known as laser refractive correction.
Two main types:
a. photorefractive keratectomy (PRK)
- outpatient procedure performed with local anaesthetic eye drops.
- laser beam reshapes the cornea by cutting microscopic amounts of tissue from the corna's outer surface.
- takes a few minutes / quick recovery
- controlled by computer
b. laser in situ keratomileusis (LASIK)
- more complex
- performed for nearsightedness
- knife removes a flap of corneal tissue, laser removes tissue underneath, and the corneal flap is replaced.
- depends on surgeon's skill (NOTE: NOWADAYS CAN BE PERFORMED ENTIRELY BY LASER AS WELL)
Both procedures have high success rates; in some cases, however, eyesight diminishes after surgery.
Impaired cornea - usually caused by disease
- corneal transplant from donor performed
- no need for type-matching
- recovery long; vision improves gradually 6-12 mths.
Clear Lens Replacement - refer to class handout - used to treat cataracts
The Human Ear p. 414- contains mechanoreceptors that translates the movement of air into a series of nerve impulses that the brain interprets as sound.
Sound waves -
travel by vibrations of air molecules
outer ear
pinna - what we'd call our ear (or ear lobe) - 'catches' sound
auditory canal - passage way between pinna and ear drum - contains hairs, sweat glands and ear wax (protection)
middle ear -
tympanic membrane (eardrum) - a membrane of thin skin and fibrous tissue that vibrates in response to sound waves, located between the outer ear and middle ear.
ossicles - three small bones of the ear - found between the ear drum and oval window. Transmit sound waves from ear drum to inner ear.
malleus (hammer) - the first of three small bones of the ear - between the tympanic membrane and incus.
incus (anvil) - second of the three bones of the ear - between the malleus and stapes
stapes (stirrup) third of three bones of the ear - between the incus and the oval window.
oval window - one of the two small openings at the end of the middle ear. Allows sound to pass to cochlea
inner ear
cochlea has fluid inside that, when moved, affect hair cells that stimulate the cochlear nerve.(view cross section, Figure 12.24 p. 416)
- hearing occurs when pressure waves move from the vestibular canal to the tympanic canal, making the
basilar membrane vibrate. This bends the hair cells between the basilar and tectorial membrane causing a nerve impulse to travel along the cochlear nerve to the brain, resulting in hearing (FYI :).
(other structures of the inner ear, the vestibule and the semicircular canals, are involved in balance and equilibrium)
semi-circular canals- three semi-circular canals are at right angles to one another, like the floor and two walls in a corner of
the room, allowing you to sense in three dimensions.
- the canals are filled with fluid and contain sensory hair cells. Changes in the position of the head are detected by
pressure exerted on the sensory receptors. Impulses sent to the brain communicate the position of the head.
spiral organ (organ of corti) - the sensory part of the cochlea in the inner ear, which responds to sound. Transmits signal to auditory (a.k.a. cochlear) nerve.
cochlear nerve (auditory nerve) - the nerve that receives the message from the spiral organ, and transmit it to the temporal lobe of the brain.
Other Parts of the ear -
Eustachian tube- connects the middle ear with the nasopharynx (throat).
- allows air pressure to equalize on both sides of the eardrum (avoids painful pressure or bursting of eardrum). - think airplanes :)
Objective 26
How we hear... (See Figure 12.23 p.415)
sounds waves enter auditory canal
tympanic membrane (a.k.a. ear drum) vibrates
vibrations pass to malleus (a.k.a. hammer), causing incus (a.k.a. anvil) and stapes (a.k.a. stirrup) to move
stapes passes vibrations to membrane of oval window
passed through to fluid within cochlea
through the spiral organ (a.k.a. organ of Corti) within the cochlea
merging with the auditory (a.k.a. cochlear) nerve
Objective 27
Disorders of the Ear
A. middle ear infections - often caused by fluid build-up behind the eardrum.
- in children, the eustachian tube is shallow and does not allow proper drainage.
-common treatment is tympanostomy tube surgery ( eustachian tube implants). Tiny plastic tubes are placed in a slit in the eardrum, allowing
fluid to drain.As the eardrum heals, the tubes are pushed out (6 mths -> 2 yrs.)
B. deafness
Two main types of deafness include:
(a) nerve deafness
- caused by damage to hair cells in the spiral organ(combined hair cells in the cochlear canal; see Fig. 12.24 p.416).
- hearing loss uneven with some frequencies more affected than others.
- typically found with aging and cannot usually be reversed.
(b) conduction deafness
- damage to the outer or middle ear affecting the transmission of sound.
- does not usually cause total loss of hearing as sound waves can also be transmitted through skull bones -> inner ear.
- hearing can be improved with hearing aids.
Hearing Aids
1. conventional
- microphone gathers sound, amplifier increases volume and receiver transmits sound to the inner ear.
- volume is user adjustable
2. programmable
- has analog circuit that can be programmed to individual's needs.
- has automatic volume control
3. digital aid
- individuals differ in levels of hearing loss at various frequencies, so different frequencies require different levels of amplification.
- digital hearing aid can shape amplification across various pitches and frequencies to suit the individual's needs.
Sound waves -
travel by vibrations of air molecules
outer ear
pinna - what we'd call our ear (or ear lobe) - 'catches' sound
auditory canal - passage way between pinna and ear drum - contains hairs, sweat glands and ear wax (protection)
middle ear -
tympanic membrane (eardrum) - a membrane of thin skin and fibrous tissue that vibrates in response to sound waves, located between the outer ear and middle ear.
ossicles - three small bones of the ear - found between the ear drum and oval window. Transmit sound waves from ear drum to inner ear.
malleus (hammer) - the first of three small bones of the ear - between the tympanic membrane and incus.
incus (anvil) - second of the three bones of the ear - between the malleus and stapes
stapes (stirrup) third of three bones of the ear - between the incus and the oval window.
oval window - one of the two small openings at the end of the middle ear. Allows sound to pass to cochlea
inner ear
cochlea has fluid inside that, when moved, affect hair cells that stimulate the cochlear nerve.(view cross section, Figure 12.24 p. 416)
- hearing occurs when pressure waves move from the vestibular canal to the tympanic canal, making the
basilar membrane vibrate. This bends the hair cells between the basilar and tectorial membrane causing a nerve impulse to travel along the cochlear nerve to the brain, resulting in hearing (FYI :).
(other structures of the inner ear, the vestibule and the semicircular canals, are involved in balance and equilibrium)
semi-circular canals- three semi-circular canals are at right angles to one another, like the floor and two walls in a corner of
the room, allowing you to sense in three dimensions.
- the canals are filled with fluid and contain sensory hair cells. Changes in the position of the head are detected by
pressure exerted on the sensory receptors. Impulses sent to the brain communicate the position of the head.
spiral organ (organ of corti) - the sensory part of the cochlea in the inner ear, which responds to sound. Transmits signal to auditory (a.k.a. cochlear) nerve.
cochlear nerve (auditory nerve) - the nerve that receives the message from the spiral organ, and transmit it to the temporal lobe of the brain.
Other Parts of the ear -
Eustachian tube- connects the middle ear with the nasopharynx (throat).
- allows air pressure to equalize on both sides of the eardrum (avoids painful pressure or bursting of eardrum). - think airplanes :)
Objective 26
How we hear... (See Figure 12.23 p.415)
sounds waves enter auditory canal
tympanic membrane (a.k.a. ear drum) vibrates
vibrations pass to malleus (a.k.a. hammer), causing incus (a.k.a. anvil) and stapes (a.k.a. stirrup) to move
stapes passes vibrations to membrane of oval window
passed through to fluid within cochlea
through the spiral organ (a.k.a. organ of Corti) within the cochlea
merging with the auditory (a.k.a. cochlear) nerve
Objective 27
Disorders of the Ear
A. middle ear infections - often caused by fluid build-up behind the eardrum.
- in children, the eustachian tube is shallow and does not allow proper drainage.
-common treatment is tympanostomy tube surgery ( eustachian tube implants). Tiny plastic tubes are placed in a slit in the eardrum, allowing
fluid to drain.As the eardrum heals, the tubes are pushed out (6 mths -> 2 yrs.)
B. deafness
Two main types of deafness include:
(a) nerve deafness
- caused by damage to hair cells in the spiral organ(combined hair cells in the cochlear canal; see Fig. 12.24 p.416).
- hearing loss uneven with some frequencies more affected than others.
- typically found with aging and cannot usually be reversed.
(b) conduction deafness
- damage to the outer or middle ear affecting the transmission of sound.
- does not usually cause total loss of hearing as sound waves can also be transmitted through skull bones -> inner ear.
- hearing can be improved with hearing aids.
Hearing Aids
1. conventional
- microphone gathers sound, amplifier increases volume and receiver transmits sound to the inner ear.
- volume is user adjustable
2. programmable
- has analog circuit that can be programmed to individual's needs.
- has automatic volume control
3. digital aid
- individuals differ in levels of hearing loss at various frequencies, so different frequencies require different levels of amplification.
- digital hearing aid can shape amplification across various pitches and frequencies to suit the individual's needs.
Objective 28.
Consider how medical treatments for visual and auditory disorders may impact a sense of exclusion, and explore the idea of mandatory
organ donation.
Ethical considerations for treatment:
• Some hearing or visually impaired individuals are unwilling to have the improvements offered by technology. Why?
– Having their impairment fixed would exclude them from the deaf/blind community of which they had been a part
– Improving their impairment could be traumatic if they feel like an outsider amongst their peers while treated as an‘impaired’ individual by the rest of the World.
– Some do not want to draw attention to themselves by wearing the equipment necessary to help them hear/see
– Long term risks of some treatments (i.e., laser)
Mandatory organ donation:
• the cornea transplant is one of the most successful transplant
surgeries; rejection is low and the operation is quick and cost effective.
• Problem is, too few corneas are available. Should mandatory donations be enforced?
Pros of mandatory donation Cons of mandatory donation
Greater supply Against religious beliefs
Improve quality of life Violation of human rights
Less impact/stress Storage issues
on family/caregivers
Consider how medical treatments for visual and auditory disorders may impact a sense of exclusion, and explore the idea of mandatory
organ donation.
Ethical considerations for treatment:
• Some hearing or visually impaired individuals are unwilling to have the improvements offered by technology. Why?
– Having their impairment fixed would exclude them from the deaf/blind community of which they had been a part
– Improving their impairment could be traumatic if they feel like an outsider amongst their peers while treated as an‘impaired’ individual by the rest of the World.
– Some do not want to draw attention to themselves by wearing the equipment necessary to help them hear/see
– Long term risks of some treatments (i.e., laser)
Mandatory organ donation:
• the cornea transplant is one of the most successful transplant
surgeries; rejection is low and the operation is quick and cost effective.
• Problem is, too few corneas are available. Should mandatory donations be enforced?
Pros of mandatory donation Cons of mandatory donation
Greater supply Against religious beliefs
Improve quality of life Violation of human rights
Less impact/stress Storage issues
on family/caregivers
