Objective 16 - Some governments try to decrease the birth rates in their countries to prevent the population from outgrowing its resources.
Demographic Transition – period of change in the growth of a population.
4 Stages:
•High birth and death rate – little growth of population (hunter/gather communities)
•High birth and lower death rate – population growing (Asia/Africa/India)
–improved standard of living
–improved medical and sanitation
–improved food sources/availability
–antibiotics
•lowering birth rate and lower death rate – still growing but less than stage 2 (Canada)
•low birth rate and low death rate – stable population. (Britian, Japan, Norway)
With the improvements in technology and contraception, countries move more efficiently from Stage 2 to Stage 3.
U.S.– took 58 years for birth rate to drop
Indonesia – 27 years
Columbia – 15 years
China - 7 years.
Why remain at Stage 2?
Lack of education, access, have to WANT less children, attitudes/cultural norms have to change.
Andhra Pradesh - Fifth largest State in India (p. 504)
·Set a quota on the number of sterilizations to be completed
·Used incentives for people who undergo sterilization (tubal ligation) – houses, land, wells, loans
·This worked to decrease the birth rate
· Do ends justify the means? Is it ok to reward poor people who have tubal ligations?
Tsunami 2006 in South-East Asia hit Andra Pradesh – women lost their children
· Reversetubal ligations were offered to those who were left childless after the tsunami
Nowadays… They are promoting spacing pregnancies, using temporary contraception (IUD, birth control pills, and condoms), and delaying
marriage.
China’s One-Child Rule
·Under the one-child policy, urban couples aren't allowed to have more than one child; overall about 63 percent of all Chinese couples
fall under the one-child rule.
·Before having a child, Chinese couples must apply for permission, called a birth permit.
·Those who follow policy are offered rewards, loans, social assistance, longer honeymoon and maternity leaves of absence.
·Those who don't comply with the one-child policy are subject to penalties including fines and confiscation of belongings.
·Family Planning Commission of China (NPFPC) offers free contraceptive methods. The most popular are IUDs and female sterilization. (Less than 10% rely on condoms, vasectomy or oral contraception)
· Abortion rate:
1 of 100 (13 million abortions annually); U.S. abortion rate:
1 in 500
· Since introducing the policy almost 35 years ago, China claims it has prevented 400 million births and the worsening of many social, environmental and economic problems.
· Other consequences: forced abortions, female infanticide, involuntary sterilizations, abandonment
Nowadays…
· After decades of controversy, Chinese leaders loosened the policy to allow any parent who is an only child themselves to have a second child.
· China has prohibited ultrasounds to determine gender and sex-selective abortions after an ultrasound.
· The smaller workforce comprised of singleton children is challenged to support two sets of aging parents; China also lacks adequate pension coverage and social welfare systems.
·The sex ratio at birth (between male and female births) is
117:100 and substantially higher than the natural baseline, which ranges between
103:100 and 107:100.
· According to a report, there will be 30 million more men than women in
2020, potentially leading to social instability, and courtship-motivated
emigration.
Objective 17 - Should we be funding methods of controlling the population (birth control) or technology supporting fertility
problems?
Population Control: The issues –
• Lack of resources in stage 2 (developing) countries
– Try to reduce birth rate –improve quality of life
– World issue
– More people affected
– Need education – this requires money
– Will governments invest in another country’s problems?
Fertility Problems: The issues –
• Toxins in environment
• Later pregnancies
– Research by private companies AND government
– People often pay-per-use
-- Less people affected
18. Trace the journey of the egg after fertilization until implantation. (p. 506-07)
· Fertilization occurs in the oviduct (fallopian tube)
· Fertilization– first stage in embryonic development, when a sperm and an egg combine to form a zygote.
· Only one sperm can fertilize an egg (the enzymes from the sperm’s acrosome digests the egg’s jelly coating)
· The egg then develops an impenetrable coat so that no other sperm can fertilize it.
· The zygote continue down the oviduct toward the uterus
· 5-10 days after fertilization, the zygote enters the uterus (meanwhile the zygote is undergoing cell division without cell growth – cleavage)
· Upon dividing, the zygote is now referred to as an embryo (0-8 weeks)
· The outer layer of the embryo cells secrete enzymes that digest part of the uterine think lining
· The embryo attaches to the endometrium (implantation). This marks the beginning of pregnancy – period when baby develops in the
uterus)
**ectopic pregnancy– embryo implants somewhere other than the uterus (oviduct, abdomen). Usually results in embryo death.
** if the egg was not fertilized, it would pass through the uterus, down through the cervix and out of the body during menstruation.
Demographic Transition – period of change in the growth of a population.
4 Stages:
•High birth and death rate – little growth of population (hunter/gather communities)
•High birth and lower death rate – population growing (Asia/Africa/India)
–improved standard of living
–improved medical and sanitation
–improved food sources/availability
–antibiotics
•lowering birth rate and lower death rate – still growing but less than stage 2 (Canada)
•low birth rate and low death rate – stable population. (Britian, Japan, Norway)
With the improvements in technology and contraception, countries move more efficiently from Stage 2 to Stage 3.
U.S.– took 58 years for birth rate to drop
Indonesia – 27 years
Columbia – 15 years
China - 7 years.
Why remain at Stage 2?
Lack of education, access, have to WANT less children, attitudes/cultural norms have to change.
Andhra Pradesh - Fifth largest State in India (p. 504)
·Set a quota on the number of sterilizations to be completed
·Used incentives for people who undergo sterilization (tubal ligation) – houses, land, wells, loans
·This worked to decrease the birth rate
· Do ends justify the means? Is it ok to reward poor people who have tubal ligations?
Tsunami 2006 in South-East Asia hit Andra Pradesh – women lost their children
· Reversetubal ligations were offered to those who were left childless after the tsunami
Nowadays… They are promoting spacing pregnancies, using temporary contraception (IUD, birth control pills, and condoms), and delaying
marriage.
China’s One-Child Rule
·Under the one-child policy, urban couples aren't allowed to have more than one child; overall about 63 percent of all Chinese couples
fall under the one-child rule.
·Before having a child, Chinese couples must apply for permission, called a birth permit.
·Those who follow policy are offered rewards, loans, social assistance, longer honeymoon and maternity leaves of absence.
·Those who don't comply with the one-child policy are subject to penalties including fines and confiscation of belongings.
·Family Planning Commission of China (NPFPC) offers free contraceptive methods. The most popular are IUDs and female sterilization. (Less than 10% rely on condoms, vasectomy or oral contraception)
· Abortion rate:
1 of 100 (13 million abortions annually); U.S. abortion rate:
1 in 500
· Since introducing the policy almost 35 years ago, China claims it has prevented 400 million births and the worsening of many social, environmental and economic problems.
· Other consequences: forced abortions, female infanticide, involuntary sterilizations, abandonment
Nowadays…
· After decades of controversy, Chinese leaders loosened the policy to allow any parent who is an only child themselves to have a second child.
· China has prohibited ultrasounds to determine gender and sex-selective abortions after an ultrasound.
· The smaller workforce comprised of singleton children is challenged to support two sets of aging parents; China also lacks adequate pension coverage and social welfare systems.
·The sex ratio at birth (between male and female births) is
117:100 and substantially higher than the natural baseline, which ranges between
103:100 and 107:100.
· According to a report, there will be 30 million more men than women in
2020, potentially leading to social instability, and courtship-motivated
emigration.
Objective 17 - Should we be funding methods of controlling the population (birth control) or technology supporting fertility
problems?
Population Control: The issues –
• Lack of resources in stage 2 (developing) countries
– Try to reduce birth rate –improve quality of life
– World issue
– More people affected
– Need education – this requires money
– Will governments invest in another country’s problems?
Fertility Problems: The issues –
• Toxins in environment
• Later pregnancies
– Research by private companies AND government
– People often pay-per-use
-- Less people affected
18. Trace the journey of the egg after fertilization until implantation. (p. 506-07)
· Fertilization occurs in the oviduct (fallopian tube)
· Fertilization– first stage in embryonic development, when a sperm and an egg combine to form a zygote.
· Only one sperm can fertilize an egg (the enzymes from the sperm’s acrosome digests the egg’s jelly coating)
· The egg then develops an impenetrable coat so that no other sperm can fertilize it.
· The zygote continue down the oviduct toward the uterus
· 5-10 days after fertilization, the zygote enters the uterus (meanwhile the zygote is undergoing cell division without cell growth – cleavage)
· Upon dividing, the zygote is now referred to as an embryo (0-8 weeks)
· The outer layer of the embryo cells secrete enzymes that digest part of the uterine think lining
· The embryo attaches to the endometrium (implantation). This marks the beginning of pregnancy – period when baby develops in the
uterus)
**ectopic pregnancy– embryo implants somewhere other than the uterus (oviduct, abdomen). Usually results in embryo death.
** if the egg was not fertilized, it would pass through the uterus, down through the cervix and out of the body during menstruation.
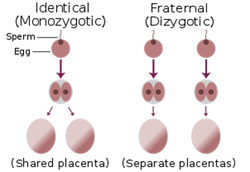
19. Twins (p. 507)
Fraternal – when more than one egg is released from the ovary or ovaries at the same time and more than one is fertilized. Offspring are as different as normal siblings.
Identical – one sperm fertilizes one egg (usual). In the early stages of development (within first 5 days), the zygote or blastocyst splits into two separate cells. Offspring will look the same and be the same sex as they have identical genetic material.
Fraternal – when more than one egg is released from the ovary or ovaries at the same time and more than one is fertilized. Offspring are as different as normal siblings.
Identical – one sperm fertilizes one egg (usual). In the early stages of development (within first 5 days), the zygote or blastocyst splits into two separate cells. Offspring will look the same and be the same sex as they have identical genetic material.
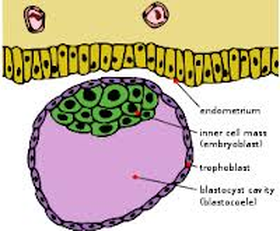
20. Stages of the embryo: morula, blastula (blastocyst), gastrula, neurula (p. 507-09)
Morula – the mass of identical cells produced as the embryo is undergoing cleavage.
Blastocyst/blastula– a hollow, fluid-filled cavity surrounded by cells. The inner cell mass in one area of the blastocyst will become the embryo.
Trophoblast- the outer layer of cells in the blastocyst that will develop into the embryonic membranes
Blastocoels – the fluid-filled cavity of the blastula.
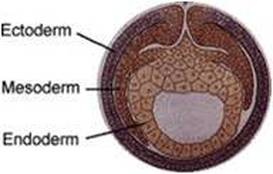
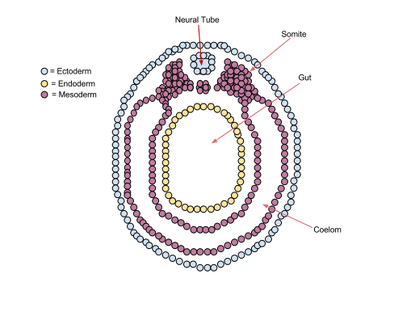
Gastrula – stage of embryonic development after the blastula in which the embryo develops distinct layers (germ layers: ectoderm, mesoderm, and endoderm).
The germ layers form during the process of gastrulation
Ectoderm –develops into the skin and nervous system
Mesoderm –develops into kidneys, skeleton, muscles, blood vessels and gonads
Endoderm – lungs and lining of the digestive tract
Neurula – stage of the embryo after the gastrula in which the nervous system begins to develop; develops from the ectoderm around the 3rd week. ·
Notochord – rod of cartiliage that arises from the mesoderm that runs along the dorsal (back) length of the body and is later replaced by bone (vertebral column)
Neural tube becomes the brain and spinal cord.
Morula – the mass of identical cells produced as the embryo is undergoing cleavage.
Blastocyst/blastula– a hollow, fluid-filled cavity surrounded by cells. The inner cell mass in one area of the blastocyst will become the embryo.
Trophoblast- the outer layer of cells in the blastocyst that will develop into the embryonic membranes
Blastocoels – the fluid-filled cavity of the blastula.
Gastrula – stage of embryonic development after the blastula in which the embryo develops distinct layers (germ layers: ectoderm, mesoderm, and endoderm).
The germ layers form during the process of gastrulation
Ectoderm –develops into the skin and nervous system
Mesoderm –develops into kidneys, skeleton, muscles, blood vessels and gonads
Endoderm – lungs and lining of the digestive tract
Neurula – stage of the embryo after the gastrula in which the nervous system begins to develop; develops from the ectoderm around the 3rd week. ·
Notochord – rod of cartiliage that arises from the mesoderm that runs along the dorsal (back) length of the body and is later replaced by bone (vertebral column)
Neural tube becomes the brain and spinal cord.
21. Primary Membranes: yolk, allantois, amnion, chorion (p. 508)
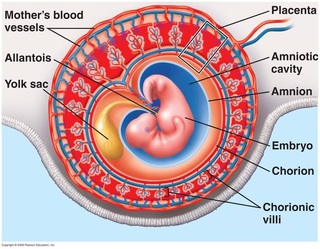
Primary membranes– not part of the embryo but supports, nourishes and protects it;
derived from germ layers.
Yolk sac –structure that surrounds the yolk (dense material that nourishes the
embryo); humans have very little yolk but they do have a yolk sac where blood
cell formation first occurs.
Allantois – the blood vessels of the allantois becomes the blood vessels of the umbilical cord; collects wastes (both yolk sac and allantois develop into umbilical cord).
Amnion – layer that completely surrounds the fetus within the chorion.
contains amniotic fluid to cushion and protect the embryo, absorbing any shock and providing a stable environment; provides a liquid environment for the developing embryo.
Chorion – origin: outer layer of the blastula. Membrane that surrounds the embryo and other membranes; has chorionic villi. It is embedded in the endometrium (uterine lining) that forms the placenta.
Primary membranes– not part of the embryo but supports, nourishes and protects it;
derived from germ layers.
Yolk sac –structure that surrounds the yolk (dense material that nourishes the
embryo); humans have very little yolk but they do have a yolk sac where blood
cell formation first occurs.
Allantois – the blood vessels of the allantois becomes the blood vessels of the umbilical cord; collects wastes (both yolk sac and allantois develop into umbilical cord).
Amnion – layer that completely surrounds the fetus within the chorion.
contains amniotic fluid to cushion and protect the embryo, absorbing any shock and providing a stable environment; provides a liquid environment for the developing embryo.
Chorion – origin: outer layer of the blastula. Membrane that surrounds the embryo and other membranes; has chorionic villi. It is embedded in the endometrium (uterine lining) that forms the placenta.
Development of Embryo
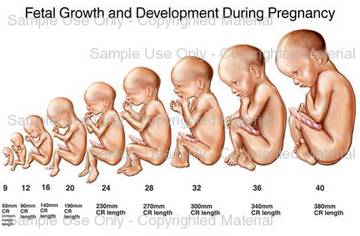
First Trimester
At four weeks, differentiated progresses - limbs, eyes and spine
8-9 weeks: first bone cells (fetus)
after 12 weeks, major organs beginning to form: liver, stomach, brain and heart
head and limbs predominant
100mm long (3 inches)
Second Trimester (weeks 13-24)
forth month, can hear heartbeat with a stethoscope
skeleton forms
brain grows rapidly, nervous system begins functioning
by 24 weeks - 300mm (~9 inches)
a fetus will not survive if born at this stage
Third trimester (weeks 25-38)
fetus - overall size increases
immune system develops
brain continues to develop and grow
eyes are open
fetus needs more calories
by the end, baby is 525mm and 3380kg
First Trimester
At four weeks, differentiated progresses - limbs, eyes and spine
8-9 weeks: first bone cells (fetus)
after 12 weeks, major organs beginning to form: liver, stomach, brain and heart
head and limbs predominant
100mm long (3 inches)
Second Trimester (weeks 13-24)
forth month, can hear heartbeat with a stethoscope
skeleton forms
brain grows rapidly, nervous system begins functioning
by 24 weeks - 300mm (~9 inches)
a fetus will not survive if born at this stage
Third trimester (weeks 25-38)
fetus - overall size increases
immune system develops
brain continues to develop and grow
eyes are open
fetus needs more calories
by the end, baby is 525mm and 3380kg
23. Umbilical Cord and Placenta (p. 510-11)
Placenta –temporary organ rich in blood vessels that develops inside the uterus in order to supply food and oxygen to the fetus via the umbilical cord. Also helps fetus get rid of wastes. Forms from the chorion once the embryo is implanted. It is fully formed by the tenth week, producing estrogen and progesterone (prevent development of new follicles and prevents menstruation by maintaining the uterine lining).
**corpus luteum produces estrogen and progesterone during the first three weeks of pregnancy, until the fetus is able to do it on its own.
Umbilical cord –a rope-like structure that connects the abdomen of the fetus to the mother’s
placenta in the uterus. A lifeline through which nutrients are received and wastes removed; prevents the mixing of mother-fetal blood.
Placenta –temporary organ rich in blood vessels that develops inside the uterus in order to supply food and oxygen to the fetus via the umbilical cord. Also helps fetus get rid of wastes. Forms from the chorion once the embryo is implanted. It is fully formed by the tenth week, producing estrogen and progesterone (prevent development of new follicles and prevents menstruation by maintaining the uterine lining).
**corpus luteum produces estrogen and progesterone during the first three weeks of pregnancy, until the fetus is able to do it on its own.
Umbilical cord –a rope-like structure that connects the abdomen of the fetus to the mother’s
placenta in the uterus. A lifeline through which nutrients are received and wastes removed; prevents the mixing of mother-fetal blood.

24. Effects of teratogens on baby (p. 511)
Teratogen – any agent that causes a structural abnormality due to fetal exposure during
pregnancy.
Cigarette smoke –constructs fetus’ blood vessels (less oxygen available than necessary); may result in lower birth weight and convulsions.
Alcohol – may cause FAS (fetal alcohol syndrome). This can affect the
brain, CNS and physical development. Lower weight, height, and head size; malformed head and face; mental
retardation and aggression/personality disorders
Prescription drugs
Thalidomide – prescribed from morning sickness in the 1950’s. Resulted in missing/deformed limbs (see above pic).
** check new medication to see if safe to take during pregnancy
Other tetratogens:
x-rays, pollutants, PCB’s (used as lubricants or to insulate electrical equipment), organic mercury compound (skincare products, drinking water)
Teratogen – any agent that causes a structural abnormality due to fetal exposure during
pregnancy.
Cigarette smoke –constructs fetus’ blood vessels (less oxygen available than necessary); may result in lower birth weight and convulsions.
Alcohol – may cause FAS (fetal alcohol syndrome). This can affect the
brain, CNS and physical development. Lower weight, height, and head size; malformed head and face; mental
retardation and aggression/personality disorders
Prescription drugs
Thalidomide – prescribed from morning sickness in the 1950’s. Resulted in missing/deformed limbs (see above pic).
** check new medication to see if safe to take during pregnancy
Other tetratogens:
x-rays, pollutants, PCB’s (used as lubricants or to insulate electrical equipment), organic mercury compound (skincare products, drinking water)

25. Process of childbirth (p. 512-13)
Gestation –length of pregnancy (9 months). Varies in mammals (20 days in mice, 21 months in an elephant)
Birth is triggered by sudden dramatic changes in hormone (estrogen and progesterone) levels.
It is believed that prostaglandins are involved (see objective 26).
Dilation stage –cervix dilates due to increased levels of oxytocin and therefore, rhythmic, uterine contractions).
Amnion breaks, releasing amniotic fluid (helps lubricate birth canal). Diameter goes from 1-2 cm to 11-12 cm before a baby can pass through. Lasts 2-20 hours
Expulsion stage –once cervix is large enough, contractions push baby from uterus out through the vagina (birth canal), head first (head rotates for ease of passage). Lasts 0.5-2 hours. Umbilical cord is clamped, tied and cut.
Placental stage –after the baby is born (10-15 minutes later) the placenta (afterbirth) and umbilical cord are expelled from the uterus via uterine contractions.
Problems: prematurity, STI, breach (rump-first) – can result in cesarian section (cut in abdomen and uterus)
Gestation –length of pregnancy (9 months). Varies in mammals (20 days in mice, 21 months in an elephant)
Birth is triggered by sudden dramatic changes in hormone (estrogen and progesterone) levels.
It is believed that prostaglandins are involved (see objective 26).
Dilation stage –cervix dilates due to increased levels of oxytocin and therefore, rhythmic, uterine contractions).
Amnion breaks, releasing amniotic fluid (helps lubricate birth canal). Diameter goes from 1-2 cm to 11-12 cm before a baby can pass through. Lasts 2-20 hours
Expulsion stage –once cervix is large enough, contractions push baby from uterus out through the vagina (birth canal), head first (head rotates for ease of passage). Lasts 0.5-2 hours. Umbilical cord is clamped, tied and cut.
Placental stage –after the baby is born (10-15 minutes later) the placenta (afterbirth) and umbilical cord are expelled from the uterus via uterine contractions.
Problems: prematurity, STI, breach (rump-first) – can result in cesarian section (cut in abdomen and uterus)
26. Hormones associated with implantation, birth and lactation: (p. 507, 510, 512-514)
Implantation:
Progesterone– first produced by the corpus luteum to prepare the uterus for the fertilized ovum and later by the
placenta to maintain pregnancy. Progesterone inhibits the development of other follicles and maintains the uterine lining.
HCG (human chorionic gonadotropin) – secreted by the trophoblast (it’s what detected by pregnancy tests). Stimulates the corpus luteum to continue to produce progesterone.
Birth is triggered by changes in hormone levels (drop in estrogen and progesterone)
Prostaglandins– may cause the release of oxytocin. Both cause the uterus to contract, signalling the beginning of labour.
Lactation –secretion or formation of breast milk in the mother.
Prolactin –released by anterior pituitary: needed for milk production; not secreted during pregnancy (high levels of estrogen and progesterone during pregnancy suppress prolactin)
Oxytocin –nerve impulse of a suckling baby stimulates the pituitary to release oxytocin. Oxytocin causes contractions in mammary lobules (lobules contain alveoli, which are sacs than contain milk)
27. Techniques used to monitor embryonic/fetal development: (p. 607, 510)
Ultrasound – sound waves bounce off the fetus and can create a black and white image. Can determines the exact location of the fetus in the uterus or detect physical abnormalities such as a missing limb, malformed heart, or cleft palate.
Amniocentesis –amniotic fluid is withdrawn from the amniotic sac, after which the fetal cells are cultured and studied. Can be used to create a
karyotype to search for genetic problems (Downs syndrome). Can occur after 14th week.
Chorionic villi sampling (CVS) – cells can be removed from the chorion (9thweek). Chorion is one of the tissues that make up the placenta. It is made of fetal cells and therefore contains genetic information. Cells are grown in culture and a karyotype is created.
Fetoscopy –direct observation of the fetus. Endoscope is inserted in a small incision in the abdomen. Enables performance of any procedures
inside the womb if necessary (remove excess fluid, blood transfusions).
Implantation:
Progesterone– first produced by the corpus luteum to prepare the uterus for the fertilized ovum and later by the
placenta to maintain pregnancy. Progesterone inhibits the development of other follicles and maintains the uterine lining.
HCG (human chorionic gonadotropin) – secreted by the trophoblast (it’s what detected by pregnancy tests). Stimulates the corpus luteum to continue to produce progesterone.
Birth is triggered by changes in hormone levels (drop in estrogen and progesterone)
Prostaglandins– may cause the release of oxytocin. Both cause the uterus to contract, signalling the beginning of labour.
Lactation –secretion or formation of breast milk in the mother.
Prolactin –released by anterior pituitary: needed for milk production; not secreted during pregnancy (high levels of estrogen and progesterone during pregnancy suppress prolactin)
Oxytocin –nerve impulse of a suckling baby stimulates the pituitary to release oxytocin. Oxytocin causes contractions in mammary lobules (lobules contain alveoli, which are sacs than contain milk)
27. Techniques used to monitor embryonic/fetal development: (p. 607, 510)
Ultrasound – sound waves bounce off the fetus and can create a black and white image. Can determines the exact location of the fetus in the uterus or detect physical abnormalities such as a missing limb, malformed heart, or cleft palate.
Amniocentesis –amniotic fluid is withdrawn from the amniotic sac, after which the fetal cells are cultured and studied. Can be used to create a
karyotype to search for genetic problems (Downs syndrome). Can occur after 14th week.
Chorionic villi sampling (CVS) – cells can be removed from the chorion (9thweek). Chorion is one of the tissues that make up the placenta. It is made of fetal cells and therefore contains genetic information. Cells are grown in culture and a karyotype is created.
Fetoscopy –direct observation of the fetus. Endoscope is inserted in a small incision in the abdomen. Enables performance of any procedures
inside the womb if necessary (remove excess fluid, blood transfusions).
